

Visual abstract
Keywords
How to Cite
Cited by




Abstract
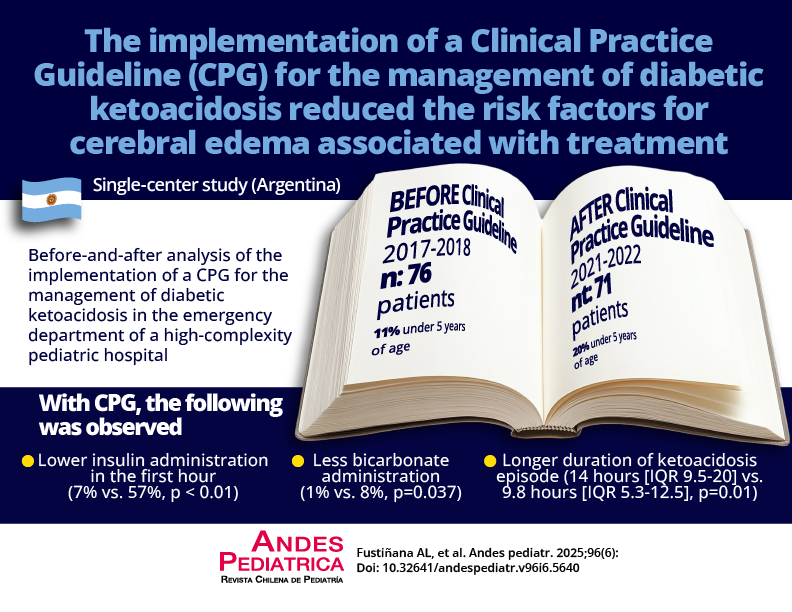
Diabetic ketoacidosis (DKA) is the leading cause of morbidity and mortality in pediatric diabetes, mainly due to cerebral edema (CE). Standardized treatment reduces the risk of CE.
Objective: To compare the duration of DKA episodes and risk factors for CE after implementing clinical practice guidelines (CPGs).
Patients and Method: A before-and-after study was conducted in children aged < 18 years with DKA admitted to the Emergency Department between 01/01/2017-12/31/2018 (PRECPG) and 01/01/2021-12/31/2022 (CPG). Patients with comorbidities were excluded. Demographic, clinical, laboratory, and treatment variables were recorded, as well as DKA episode duration and CE risk factors (early insulin administration within the first hour and use of bicarbonate for correction). Survival analysis and Cox proportional hazards modeling were performed, reporting hazard ratios (HR) and 95% confidence intervals (95% CI).
Results: A total of 76 children in PRE-CPG and 71 in CPG were included. The CPG group showed a higher proportion of diabetic onset (70% vs. 34%, p < 0.01). Episode duration was longer in the CPG group than the PRE-CPG one (14 h [IQR 9.5-20] vs. 9.8 h [IQR 5.3-12.5]; p = 0.01, respectively). The resolution curve was faster in the PRE-CPG group (HR 0.62; 95% CI 0.43-0.90; p = 0.017). Compared with the PRE-CPG group, the CPG one showed lower insulin administration in the first hour (7% vs. 57%, p < 0.01) and lower bicarbonate use (1% vs. 8%, p = 0.037).
Conclusions: The implementation of the CPG was associated with longer DKA episodes and a reduction in treatment-related CE risk factors, such as early insulin administration and bicarbonate use.

This work is licensed under a Creative Commons Attribution 4.0 International License.
Copyright (c) 2025 Revista Chilena de Pediatría